The Trump effect on high drug prices
US President Donald Trump said on May 11 that he wants prices of drugs sold in the US to reflect the cheapest prices globally. ST PHOTO: KUA CHEE SIONG
PUBLISHED Jun 09, 2025, 05:00 AM
Thanks for sharing!
SINGAPORE – If US President Donald Trump had his way, the price of medication in the US would fall drastically – while the rest of the world would end up paying more, possibly a lot more.
His declaration on Facebook on May 11 that he wants prices of drugs sold in the US to reflect the cheapest prices globally sent shares of large pharmaceutical companies tumbling across the world, with several losing 3 per cent or more of their stock market value within hours.
But the steep plunge reversed just as abruptly once the executive order signed by Mr Trump on the morning of May 12 was made public. This was because the order lacked details, which led some observers to note that there was more bark than bite in his words .
Today, the US, with 340 million people, or less than 5 per cent of the world’s population, spends about US$5 trillion (S$6.5 trillion) a year on healthcare – and accounts for about 45 per cent of global pharmaceutical sales.
One reason is that people in the US consume more medicine per capita than the rest of the world. Since they use more, they buy more, and hence spend more on drugs.
Another reason, which is what upsets Mr Trump, is that prices of drugs, particularly those still under patent, are generally much higher in the US than anywhere else in the world.
Pharmaceutical companies say the high prices paid in the US allow consumers there to be among the first to get any new treatments.
Mr Trump gave the example of a “fat drug”, without naming it, that costs 10 times more in the US than in some other countries.
He was likely referring to the highly popular diabetes drug Ozempic, which is also prescribed for weight loss under the trade name Wegovy.
A 2023 comparison of prices by the independent Peterson-KFF Health System Tracker found “the list price for one month of Ozempic in the US (US$936) is over five times that in Japan (US$169), and about 10 times more than in Sweden, the United Kingdom, Australia and France”.
Drug companies have historically priced their products differently in different countries. Generally, richer countries tend to pay more than poorer countries with lower purchasing power.
The Singapore Association of Pharmaceutical Industries (Sapi) told The Straits Times: “Pharmaceutical companies work with local governments and healthcare systems to offer flexible and tailored pricing solutions based on each country’s needs, helping make medicine and vaccines more affordable and accessible, especially in countries with fewer resources.
“Tiered pricing is one of the most effective and sustainable ways in which pharmaceutical companies help to improve and sustain access to medicine globally.”
The cost of medication in Singapore, for example, is much higher than in neighbouring countries, so it is not uncommon for people to cross the Causeway, where savings could be significant, to buy their medicine.
Having said that, rich countries also can get drugs more cheaply because of their buying power and ability to negotiate better prices.
Australia, for example, sets a cap on the price of drugs it allows to be sold in the country. This can mean, however, that fewer drugs are available in Australia – compared with Singapore, for instance – as some pharmaceutical companies will refuse to sell at the designated prices.
Even within the US, drug prices do vary. But the US does not benefit from its large purchasing power because the prices were negotiated individually between drug companies and their buyers – typically insurance companies, pharmacy chains and hospitals.
Mr Trump’s executive order states: “The inflated prices in the United States fuel global innovation while foreign health systems get a free ride.”
Associate Professor Wee Hwee Lin of the Saw Swee Hock School of Public Health said one of the main reasons drug prices are so high in the US is that there has been no direct price control mechanism, unlike in many other developed countries.
Drugs have to prove only safety, efficacy and quality – but not cost-effectiveness, as is required in some other countries. She added that many pharmaceutical companies also choose to launch in the US first, as they can command the highest prices there, thus setting the bar for the rest.
This may change with the passage of the Inflation Reduction Act (IRA) in 2022, which, for the first time, empowered Medicare to negotiate prices directly with drug companies.
It had previously been legally prohibited from negotiating drug prices under a “non-interference clause” in the Medicare Prescription Drug, Improvement and Modernisation Act 2003.
Medicare, the national insurance for people over 65 and those with disabilities, is the single largest payer of healthcare in the US, and covers more than 55 million Americans for outpatient prescription drugs.
Said Prof Wee, whose teaching areas include pharmacy practice: “Prior to the IRA, Medicare was explicitly prohibited from negotiating prices directly with pharmaceutical companies. Therefore, drug prices in the US may be considered to be market-based pricing, based on supply and demand.”
Even with the passing of the IRA, the cheaper negotiated prices will start to take effect only from 2026.
Since the IRA was passed, Medicare has completed negotiations on 10 drugs that alone cost it US$50.5 billion in 2022, or about 20 per cent of its gross total drug spending . The drugs, which are used to treat chronic diseases such as diabetes and cancer, will have maximum prices that are 38 per cent to 79 per cent cheaper from January 2026.
The IRA allows it to negotiate prices for 10 drugs in the first year, 15 in the next two years, and 20 a year thereafter.
It has embarked on negotiations for the next 15 drugs, also for chronic diseases like diabetes, cardiovascular disease and cancer, to take effect from January 2027. Ozempic is one of them.
Legal challenges have been mounted against the drug negotiation programme. According to a US Congress report, “beginning in June 2023, several pharmaceutical manufacturers and trade associations filed lawsuits in various federal district courts alleging that the programme was unconstitutional”.
So far, most have failed, but some court cases are still ongoing. In contrast, some Congress members want to expand the programme to more drugs in the market.
Prof Wee said most other developed countries exert some control over drug prices by government intervention that will “thus introduce market failure”.
Britain’s National Institute for Health and Care Excellence is a forerunner of healthcare technology assessment, which looks at whether the benefits of new treatments justify the price asked for.
If they do not, the treatment would not be recommended to the National Health Service, which pays for almost all drugs used in the country.
Many other countries in Europe and Asia have similar agencies to control the cost of new and expensive treatments.
Singapore recently tasked the Agency for Care Effectiveness with studying new treatments and deciding if they provide value for money – changing the nation from being a passive price taker to one that has some clout in deciding the “correct” pricing for the benefits from a treatment.
It resulted in the Cancer Drug List, a list of treatments approved for insurance coverage, which has led to across-the-board savings of about 30 per cent in the public sector. At the upper ranges, the prices of cancer drugs fell by as much as 60 per cent.
Pharmaceutical companies are still free to sell their cancer drugs at any price – but unless their price to the public sector is deemed cost-effective, they cannot be covered by MediShield Life or Integrated Shield Plan insurance, which pays for the vast majority of cancer treatments here.
Singapore, being a small market, continues to pay a lot more than places like Australia, Taiwan and South Korea for many other drugs.
Prof Wee pointed out that another major reason for the high drug prices in the US is the use of middlemen such as pharmacy benefits managers (PBMs). She said PBMs were originally intended to streamline procurement processes and help drive down costs for insurers and employers.
“However, over time, many unintended consequences arose. For example, there is a lack of transparency as regard the amount of rebates PBMs receive from the pharmaceutical companies relative to the list price,” she said.
On the day the US President’s executive order was signed, Mr Stephen J. Ubl, president and chief executive of the Pharmaceutical Research and Manufacturers of America, released a statement saying: “The US is the only country in the world that lets PBMs, insurers and hospitals take 50 per cent of every dollar spent on medicine.
“The amount going to middlemen often exceeds the price in Europe. Giving this money directly to patients will lower their medicine costs and significantly reduce the gap with European prices.”
Prof Wee said the influence of PBMs goes beyond just taking a big cut from the sale of drugs: “PBMs may purchase based on how much rebate they can obtain rather than what is the least-cost option. Many of the PBMs are also owned by insurance companies.
“It is not clear how the financial interests of the insurance companies are prioritised over cost savings or patient outcomes.”
Many drug companies argue that a large drop in their revenue could affect their ability to research and develop new treatments, which would be a sad loss to the world. However, there is no evidence to suggest this would actually happen.
Mr Trump, who has not mentioned the Medicare programme, nevertheless wants drugs in the US to be sold at the “most-favoured-nation price”. If that happens, prices of drugs elsewhere could go up as a result.
The order said: “My administration will take immediate steps to end global freeloading and, should drug manufacturers fail to offer American consumers the most-favoured-nation lowest price, my administration will take additional aggressive action.”
However, it did not spell out what such aggressive actions might be.
Furthermore, Mr Trump had tried something similar in his first term in office, only to be blocked by the courts. Most attempts to control drug prices will need congressional approval – something that could take years to achieve, if at all possible.
Mr Trump ordered his Secretary of Health and Human Services, Mr Robert F. Kennedy Jr, to establish a mechanism through which American patients can buy their drugs directly from manufacturers, bypassing middlemen.
This sounds promising on paper, as it would cut the price of drugs by half. But in reality, it is far more complex. If the current intermediaries between drug company and patients are removed, some other mechanism needs to take their place to ensure drugs get to patients. It might cut the price, but there would certainly be some distribution cost.
Mr Trump also suggested importing “prescription drugs on a case-by-case basis from developed nations with low-cost prescription drugs”. Even if the laws in the US can be amended to allow for this, the quantities imported are unlikely to be large enough to move the needle.
Prof Wee said that to systematically bring down the prices at which drugs are sold, the US first needs to define the set of countries that it will refer to for international reference pricing – and whether this is based on the list price or the net amount paid after negotiations, including volume discounts.
While list prices are readily available, negotiated prices are usually kept confidential.
She added that the US would also need to conduct health technology assessments to decide on what drug pricing is justifiable, at a national level. Any moves in this direction will certainly be challenged as unconstitutional, as it could prevent patients from assessing treatments deemed not to provide value for money.
In contrast, many countries in Europe and Asia, including Singapore, are willing to forgo access to new therapies if they are found to be too costly for the additional benefits provided.
In spite of the difficulties in implementing Mr Trump’s directive, his declaration of war against high drug costs in the US is likely to result in some price reduction.
Most industry experts expect pharmaceutical companies to reduce prices somewhat in an effort to allay his wrath. This will be especially for drugs that are nearing the end of their patent – so that Mr Trump can declare his move a success.
Prof Wee said it is “hard to say at the moment how the pharmaceutical companies will respond”. Should there be significant cuts in drug prices in the US, she anticipates a chain effect, which will lead to a new equilibrium in pricing globally, including in Singapore.
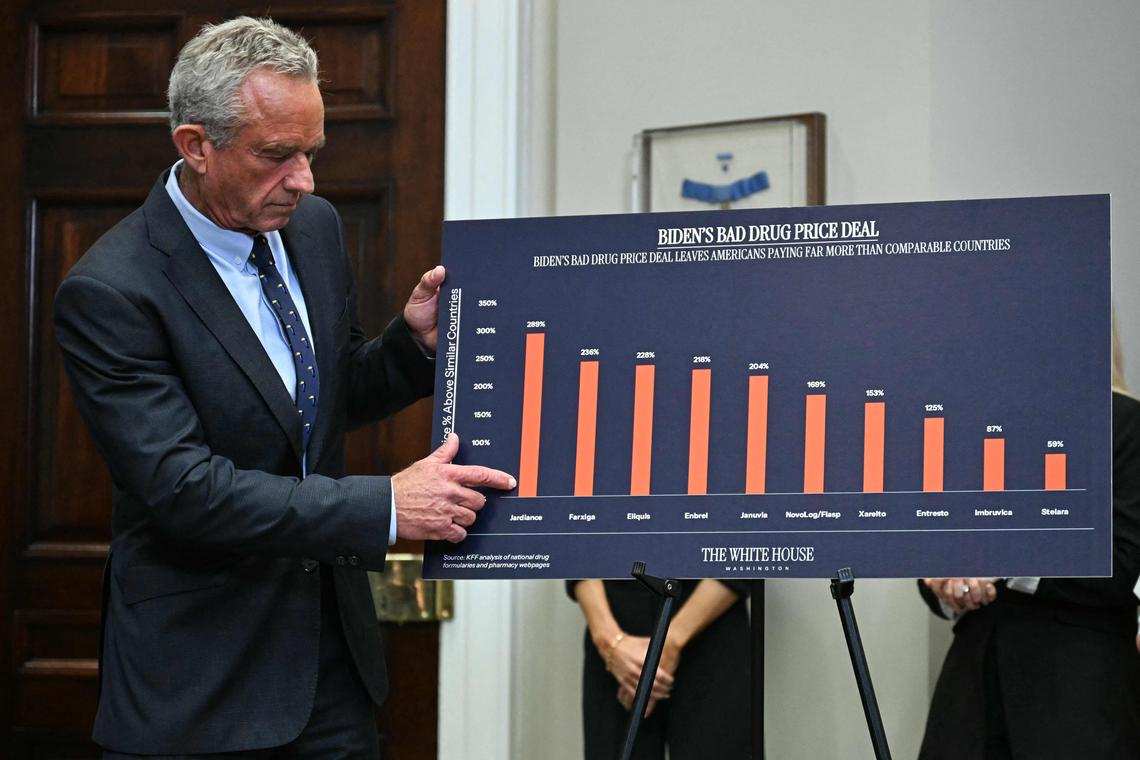
US Secretary of Health and Human Services Robert F. Kennedy Jr at a news conference about prescription drug prices at the White House on May 12. PHOTO: AFP
Going forward, exactly what will happen remains anybody’s guess.
But should the US government try to impose severe price cuts, the drug companies will likely take legal action to block such moves, given that billions of dollars are at stake. And pharmaceutical companies have deep pockets – with the top handful each raking in revenues in excess of US$50 billion in 2024.
Mr Trump’s diatribe on high drug prices in the US appears to target Europe. Referring to how countries there “force” pharmaceutical companies to cut the cost of drugs, he said “the European Union has been brutal, brutal. And the drug companies actually told me stories, it was just brutal”.
So, rather than going after the pharmaceutical industry directly, he just might penalise countries that he feels are “suppressing” drug prices to the detriment of the US.
Mr Trump is known for doing the unexpected, such as linking a 20 per cent tariff on goods from China to the inflow of fentanyl to the US. So, the penalty could be anything, including higher tariffs on totally unrelated goods to something no one has even thought about.
Any changes, big or small, in drug prices in the US will likely have some spillover effect for Singapore.
Ms Poh Hwee Tee, president of Sapi, told ST: “While it is too early to determine the full extent of the impact of the US government’s most-favoured-nation executive order, Sapi and its members are closely monitoring the developments and remain committed to working in close partnership with the Ministry of Health and other stakeholders to identify and address any potential challenges.
“Our focus remains on supporting Singapore’s healthcare ecosystem and working collaboratively with stakeholders to ensure sustainable access to innovative medicine and vaccines for patients in Singapore.”
Singapore spends about $1 billion a year on medicine. If prices were to go up by, say, 20 per cent across the board, that would be an additional $200 million a year.
While this might not amount to much for government coffers and much of the price increase for subsidised patients might be cushioned by higher subsidies, the increase may be significant for private patients.
A reassuring thought is that any increase in prices will affect only drugs that are still under patent. A lot of commonly used drugs here for conditions like diabetes, high cholesterol and blood pressure, are generic, and hence cheap. There is unlikely to be any impact on these.
Join ST's WhatsApp Channel and get the latest news and must-reads.
Thanks for sharing!
……Read full article on The Straits Times - Singapore
America Business Health Singapore

One-stop lifestyle app dedicated to making life in Singapore a breeze!



 English
English 简体中文
简体中文
Comments
Leave a comment in Nestia App